DERM-SUCCESS Prospective Skin Cancer Validation Study1,2
22 Primary Care Study Sites (18 U.S. and 4 Australia)
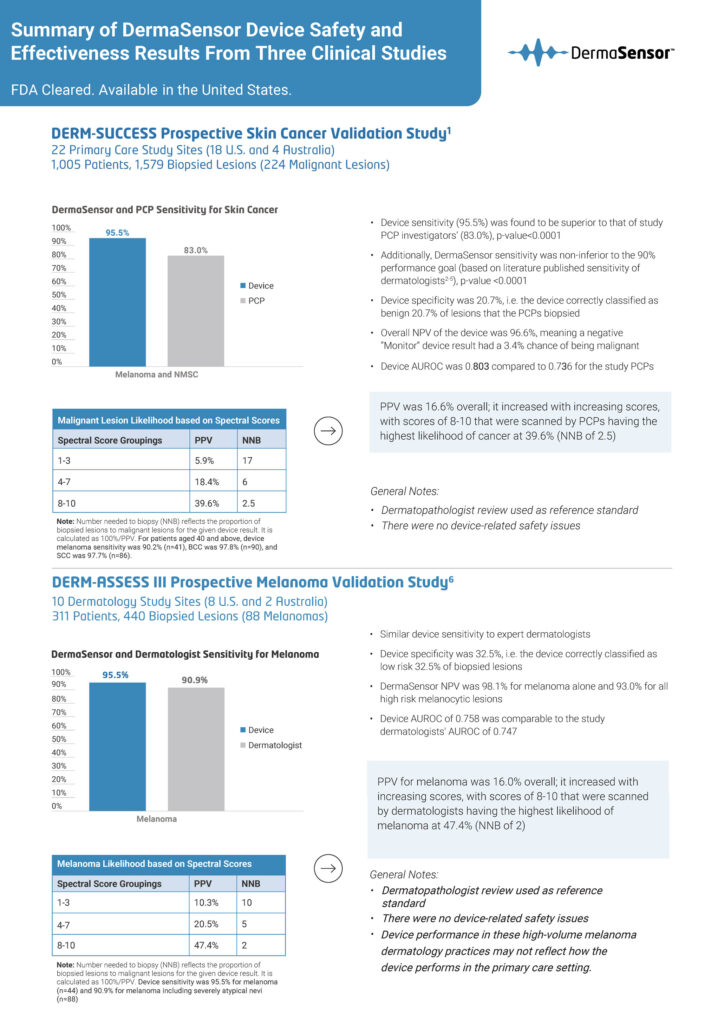
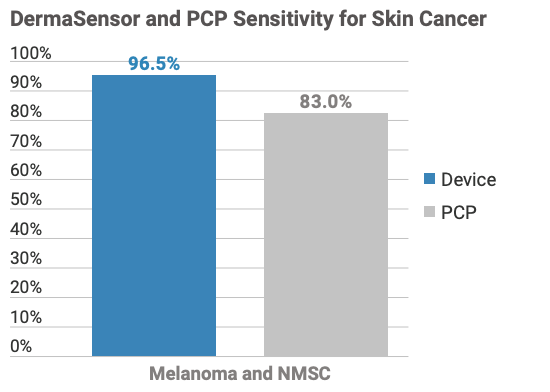
1,005 Patients, 1,579 Biopsied Lesions (224 Malignant Lesions)
- Device sensitivity (95.5%) was found to be superior to that of study PCP investigators’ (83.0%), p-value<0.0001
- Additionally, DermaSensor sensitivity was non-inferior to the 90% performance goal (based on literature published sensitivity of dermatologists3-6), p-value <0.0001
- Device specificity was 20.7%, i.e. the device correctly classified as benign 20.7% of lesions that the PCPs biopsied
- Overall NPV of the device was 96.6%, meaning a negative “Monitor” device result had a 3.4% chance of being malignant
- Device AUROC was 0.803 compared to 0.726 for the study PCPs
General Notes:
- Dermatopathologist review used as reference standard
- There were no device-related safety issues
DERM-ASSESS III Prospective Melanoma Validation Study7
10 Dermatology Study Sites (8 U.S. and 2 Australia)
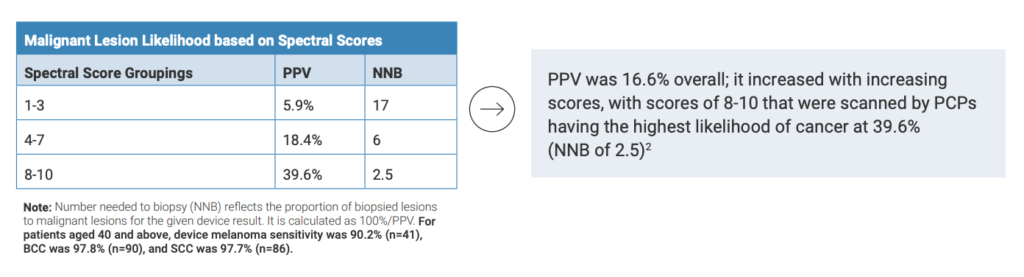
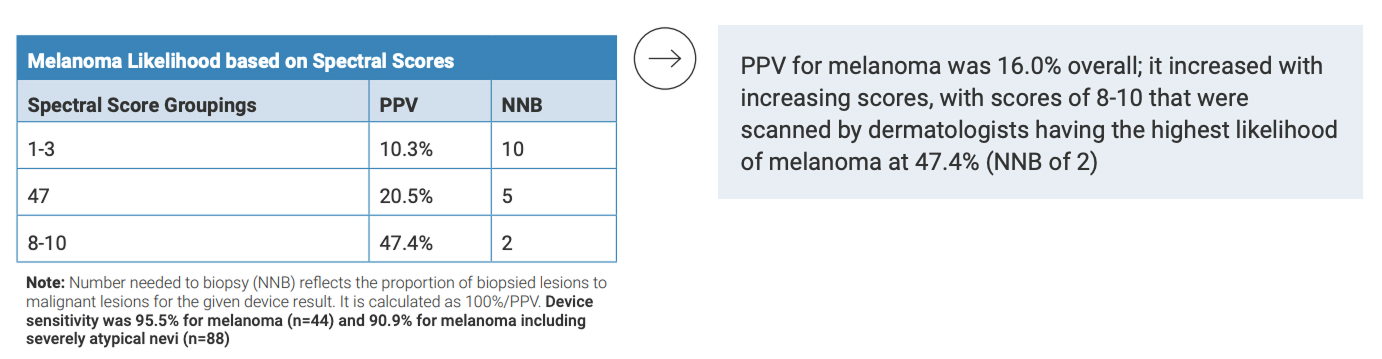
311 Patients, 440 Biopsied Lesions (88 Melanomas)

- Similar device sensitivity to expert dermatologists
- Device specificity was 32.5%, i.e. the device correctly classified as low risk 32.5% of biopsied lesions
- DermaSensor NPV was 98.1% for melanoma alone and 93.0% for all high risk melanocytic lesions
- Device AUROC of 0.758 was comparable to the study dermatologists’ AUROC of 0.747
General Notes:
- Dermatopathologist review used as reference standard
- There were no device-related safety issues Device performance in these high-volume melanoma dermatology practices may not reflect how the device performs in the primary care setting
DERM-SUCCESS Prospective Clinical Utility Study8
108 U.S. Board Certified Primary Care Providers
Over 10,000 lesion assessments

- PCP device use resulted in a significant improvement in
both management and diagnostic sensitivity compared to
standard of care alone; physician false negative referrals
decreased by half, from 18.0% to 8.6% - PCPs’ AUROC was 0.762 when aided by the device and was 0.708 with standard of care alone
- Nearly all (99%) of PCP participants reported the device would provide at least one benefit, including:
- “Detecting more skin cancer” (82%)
- “Providing you with greater confidence in your clinical assessments and management decisions” (81%)
- “Helping you to prioritize the risk level of concerning lesions to prioritize patient management, e.g. a prioritized dermatology referral” (72%)
- Increasing your frequency of assessing patients for skin cancer” (63%)
Indications for Use
The DermaSensor device is indicated for use to evaluate skin lesions suggestive of melanoma, basal cell carcinoma, and/or squamous cell carcinoma in patients aged 40 and above to assist in the decision regarding referral of the patient to a dermatologist. The DermaSensor device should be used in conjunction with the totality of clinically relevant information from the clinical assessment, including visual analysis of the lesion, by physicians who are not dermatologists. The device should be used on lesions already assessed as suspicious for skin cancer and not as a screening tool. The device should not be used as the sole diagnostic criterion nor to confirm clinical diagnosis of skin cancer.
Indicated User Considerations
The DermaSensor FDA pivotal validation study (DERM-SUCCESS) included 1,579 lesions biopsied by 22 primary care study centers, and a supplemental melanoma validation study
(DERM-ASSESS III) was conducted with biopsied lesions by 10 dermatology study centers. Note that the device indications for use describes non-dermatologist physicians since the FDA’s clearance was based on the benefit-risk evaluation for physicians who are not already experts in the clinical diagnosis and management of skin cancer.
Risks
False-positive and false-negative device results may lead to unnecessary referrals or to a malignant skin lesion not being correctly referred, respectively. For the more clinically harmful risk, a false negative device result, the DERM-SUCCESS study found the overall device sensitivity to be 95.5%, with a lower bound of 91.7%. While the device can produce false negative results, as does gold standard dermatopathology, when the device result is used to aid PCPs in their referral decisions, the reader study showed that the device decreases PCPs’ false negatives by half, with the PCPs’ false negative rate decreasing from 18.0% without device use to 8.6% with device use.
References
- Merry SP, Chatha K, Croghan I, Nguyen VL, McCormick B, Leffell D. Clinical Performance of Novel Elastic Scattering Spectroscopy (ESS) in Detection of Skin Cancer: A Blinded, Prospective, Multi-Center Clinical Trial. J Clin Aesthet Dermatol 2023 April: 16(4 Suppl): s16
- Data on File
- Carli P, Nardini P, Crocetti E, De Giorgi V, Giannotti B. Frequency and characteristics of melanomas missed at a pigmented lesion clinic: a registry-based study. Melanoma Res 2004;14(5):403-407.
- Soyer H, Argenziano G, Zalaudek I, Corona R, Sera F, Talamini R, et al. Three point checklist of dermoscopy. A new screening method for early detection of melanoma. Dermatology. 2004;208:27-31.
- Stanganelli I, Serafini M, Bucch L. A cancer-registry-assisted evaluation of the accuracy of digital epiluminescence microscopy associated with clinical examination of pigmented skin lesions. Dermatology. 2000;200(1):11-16.
- Dinnes J, Deeks JJ, Grainge MJ, et al. Visual inspection for diagnosing cutaneous melanoma in adults. Cochrane Database of Systematic Reviews. 2018;12:CD013194.
- Hartman RI, Trepanowski N, Chang MS, Tepedino K, Gianacas C, McNiff JM, Fung M, Braghiroli NF, Grant-Kels JM, Multicenter Prospective Blinded Melanoma Detection Study with a Handheld Elastic Scattering Spectroscopy Device, JAAD International (2023), doi:
https:// doi.org/10.1016/j.jdin.2023.10.0 - Seiverling EV, Agresta T, Cyr P, Caines L, Nguyen VL, Chatha K, Siegel DM. Clinical Utility of an Elastic Scattering Spectroscopy Device in Assisting Primary Care Physician’s Detection of Skin Cancers. J Clin Aesthet Dermatol 2023 April: 16(4 Suppl): s16-17.